Benign Paroxysmal Positional Vertigo (BPPV)

When you observe the surroundings spinning rapidly, many individuals may attribute it to Meniere’s disease. However, it could also be the result of an imoerceptible “ear stone” (also called otoconia). Benign Paroxysmal Positional Vertigo (BPPV) is a condition that impacts the balance system within the inner ear. It is the most prevalent peripheral vestibular disorder, comprising approximately 60% of all instances of peripheral vertigo and 25%-33% of all instances of vertigo. It has the potential to affect individuals of any age.
Content
- Why do we have ear stone?
- Classification of BPPV
- 3 major characteristics of BPPV
- What to do during an episode of BPPV?
- Does BPPV resolve on its own?
- What tests should be done when experiencing vertigo?
- BPPV treatment: Canalith Repositioning Maneuver
- Post-Canalith Repositioning Precautions
- Differentiating between Ménière's Disease and BPPV
- Recurrence rate and prevention of BPPV
Anterior Cruciate Ligament Injury: Causes, Diagnosis, and Treatment
Why do we have ear stone?
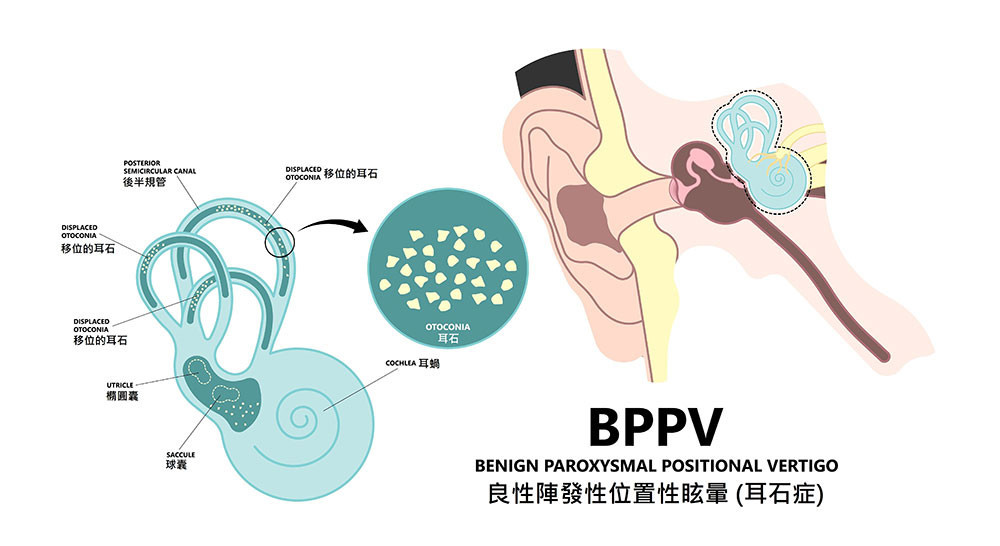
The ear serves not only as an auditory organ but also as a vital component of our balance system. Within the inner ear, there are structures responsible for sensing and regulating body balance, such as the utricle and saccule. These structures are connected to three semicircular canals that are linked to the cochlea in the inner ear and play a vital role in maintaining our body’s equilibrium balance.
In the event of a head impact, the delicate membranes inside the semicircular canals can become dislodged, forming ear stones (also called otoconia or canaliths) , which are tiny crystals of calcium carbonate. These ear stones float within the fluid-filled canals. When a person with BPPV changes the position of their head, such as when lying down, turning in bed, or looking up, the displaced ear stone may come into contact with the nerve fibres that transmit signals to the brain, interrupting the normal transmission of these signals. As a result, the brain may issue inaccurate commands to the eye muscles, leading to a sensation of objects spinning and brief episodes of intense vertigo. These episodes typically last less than one minute.
Classification of BPPV
BPPV can be classified into two types based on its etiology: idiopathic (spontaneous) and secondary.
Idiopathic BPPV
The cause is unknown and accounts for approximately 50%-97% of all cases.
Secondary BPPV
Occurs as a result of other otologic or systemic diseases, such as Meniere’s disease, vestibular neuritis, sudden sensorineural hearing loss, middle ear infection, head trauma, migraines, post-surgical (otologic or otoneurosurgical procedures, oral and maxillofacial surgery, orthopaedic surgery, etc), and the use of ototoxic medications.
Characteristics of BPPV
Benign
Benign paroxysmal positional vertigo (BPPV) is a non-life-threatening condition that can be treated and has the potential to resolve on its own. Most patients experience improvement within a few days or weeks.
Paroxysmal
The episodes of dizziness caused by BPPV are usually brief, lasting only a few seconds to a few tens of seconds, rarely exceeding one minute. Although the episodes are short-lived, they can occur multiple times and recur, causing frustration.
Positional
"Positional" refers to the fact that the episodes of dizziness are triggered by changes in head and neck position. Sometimes, patients may feel a spinning sensation when resting, getting up, or turning in bed. This sensation may be accompanied by nausea and a sense of vomiting.
What to do during an episode of BPPV?
During an episode of BPPV, individuals may experience a spinning sensation, with the surroundings appearing to rotate. Symptoms such as nausea and vomiting may also accompany the dizziness. Although each episode of BPPV-induced vertigo lasts only a few seconds to one minute, it can still have a significant impact on daily life. Some individuals experience BPPV episodes whenever they get out of bed or change positions, which can lead to a fear of sleeping and greatly affect their quality of life. BPPV patients typically have specific positions or movements that trigger their dizziness, and they should avoid rapid head movements or sudden changes in head position, especially when getting up. When feeling dizzy, it is recommended to use your hands to hold onto nearby walls or objects until the symptoms subside. During an episode, BPPV patients need to rest more and avoid driving to prevent accidents.
Does BPPV resolve on its own?
In some cases, partially dislodged ear stones will be gradually absorbed by the body, and patients may recover on their own within a few weeks or months. However, if the symptoms persist or significantly affect daily life, it is advisable to seek early medical attention to rule out other possible conditions.
What tests should be done when experiencing vertigo?
When experiencing vertigo, it is essential to consider various factors that could be causing the symptoms. BPPV is a common ear problem that can occur after a head injury. However, other conditions can cause vertigo, such as vestibular migraines, vestibular neuritis, or insufficient blood supply to the brain. To determine the cause of dizziness, doctors rely on a combination of medical history and physical examination. They may also perform vestibular function and hearing tests to assess the nature of the dizziness. In some cases, additional tests like a head magnetic resonance imaging (MRI) or a computed tomography (CT) scan may be necessary to gather more information and make an accurate diagnosis.
BPPV treatment: Canalith Repositioning Maneuver
The Canalith Repositioning Maneuver is a procedure performed in a clinical setting to treat vertigo caused by BPPV. In this procedure, the doctor assists the patient in moving their head to reposition the displaced ear stone. By utilizing the force of gravity, the ear stones are guided away from the affected nerves and back into the utricle, thereby stopping the dizziness symptoms. In most cases, one repositioning is sufficient. If the initial attempt is unsuccessful, another repositioning can be attempted after one week. There is no medication specifically for BPPV, but patients are advised to stay hydrated and maintain proper fluid balance within the inner ear to help prevent the ear stone from lingering on the nerves and reduce the chances of vertigo.
Post-Canalith Repositioning Precautions
-
Sit quietly for at least half an hour after the maneuver:
After the repositioning maneuver, some patients may experience more intense dizziness reactions and, in some cases, even vomiting. Sitting quietly for at least half an hour helps minimize the risk of the successfully repositioned ear stones becoming dislodged again.
-
Raise the head of the bed for three days:
To prevent the ear stone from shifting back out of place after repositioning, it is recommended to elevate the head of the bed by 45 degrees for three days following the procedure.
-
Avoid vigorous exercise for two weeks:
To prevent the ear stones from dislodging again, it is important to avoid activities such as tilting the head, shaking the head, jumping, or any vigorous movements for two weeks.
-
Start walking and getting out of bed as early as possible
It is beneficial to begin walking and getting out of bed as soon as possible after the procedure. However, if symptoms recur, seeking timely medical attention and revisiting the clinic for a follow-up appointment is important.
Differentiating between Ménière's Disease and BPPV
If the vertigo is severe, lasts for more than twenty minutes, and is accompanied by tinnitus and hearing loss, it is characteristic of Ménière's disease, which is a type of ear fluid imbalance. Ménière's disease is often caused by increased pressure of the inner ear fluid (endolymph) within the semicircular canals. This increased pressure can compress the delicate vestibular hair cells in the inner ear, leading to erroneous signals being sent to the brain and resulting in dizziness. The excess fluid can also exert pressure on the auditory hair cells, causing symptoms such as tinnitus and a feeling of ear fullness. Recurrent episodes of Ménière's disease may gradually lead to hearing loss. Treatment options for Ménière's disease include reducing salt intake to prevent fluid accumulation and, in some cases, using diuretic medications to minimize episodes.
| BPPV | Ménière's Disease | |
| Definition | A vestibular disorder characterized by the displacement of calcium crystals (ear stones) within the inner ear. | An inner ear disorder that affects the fluid balance in the inner ear. |
| Symptoms | Intense, brief episodes of vertigo triggered by head movements No associated hearing loss No ear fullness/pressure No persistent tinnitus | Severe, prolonged dizziness with vertigo Fluctuating hearing loss, often affecting one ear Feeling of fullness/pressure in the affected ear Persistent tinnitus |
| Age of onset | Can occur at any age | Commonly affects young to middle-aged |
Recurrence rate and prevention of BPPV
BPPV has a high recurrence rate. Epidemiological studies indicate that the recurrence rate of BPPV within one year is approximately 15%, and within 5 years, it is around 50%. After recovering from BPPV the main challenge for patients is how to prevent its recurrence. Here are the 3 key methods for preventing the recurrence of BPPV:
Improve sleep and avoid staying up late
Research has shown that a significant number of BPPV patients suffer from insufficient sleep, and inadequate sleep can increase the risk of ear stones becoming dislodged and causing BPPV.
Seek early treatment for tinnitus and hearing loss
Tinnitus and hearing loss are often associated with inner ear issues, and loose or dislodged ear stones can contribute to BPPV. Timely treatment for these conditions can help prevent BPPV.
Avoid overexertion
Some patients experience a sudden onset of BPPV after overexertion. Overexertion can lead to the dislodgement of ear stones, eventually causing BPPV.
Enhance nutrition and boost the immune system
Research suggests that some patients exhibit symptoms such as cold, malnutrition, and weakened immune system before the onset of BPPV.



Our Team
Virtus Otorhinolaryngology Specialists
More:
-
Specialty - Otorhinolaryngology